India Wants To Eliminate Malaria, But Deadlier Mosquito-Borne Diseases Rising

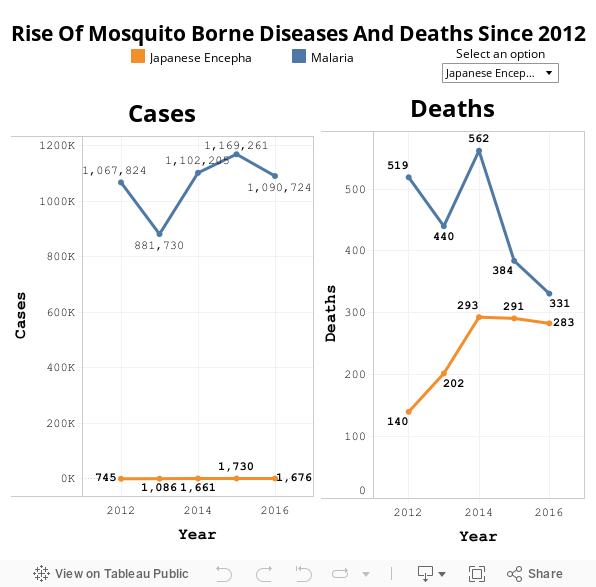
Even as India targets the elimination of malaria by 2030, other deadlier mosquito-borne diseases have been spreading rapidly nationwide. Between 2012 and 2016, there has been a 300% rise in the cases of chikungunya, dengue followed, at 157% and Japanese encephalitis, at 124%.
Cases of malaria alone rose by 2% over the same period.
Source: National Vector Borne Disease Control Programme, Central Bureau of Health Intelligence
On July 12, 2017, the national strategic plan for malaria elimination (2017-22) was launched by the union minister of health and family welfare, J P Nadda. It sets elimination targets for different parts of the country depending on the prevalence of malaria there. The plan is to oust the disease by 2027 and maintain the status till 2030 and beyond.
To be declared malaria-free, a country has to report zero incidence for at least three years.
India recorded 89% of total malaria incidence in South East Asia in 2016 but it has brought down its morbidity and mortality, stated the national strategic plan for malaria elimination. The country has more than halved the number of malaria cases, from 2 million in 2000 to 1 million in 2016.
There were 1,090,724 cases of malaria in 2016, of which 331 proved fatal, in 2016.
Here is IndiaSpend’s analysis of the challenges India will face in eliminating malaria.
Dengue cases 1/10th of malaria, but causes nearly as many deaths
Dengue is a viral disease spread by the Aedes mosquito and in severe cases can lead to a fatal drop in blood platelets causing multiple organ failure. In 2012, 50,022 cases of dengue were reported; this number grew to 129,166 in 2016, according to figures by the National Vector Borne Disease Control Program (NVBDCP).
Dengue caused 242 deaths in 2012 and 245 in 2016, comparable to the 331 deaths in 2016 due to malaria. This is despite the fact that the dengue affected one-tenth the number of people who had malaria.
Chikungunya, which causes debilitating joint pains and is also spread by the Aedes mosquito, affected 15,977 people in 2012 and 64,054 in 2016. Even though government records say that the disease has yet to prove fatal, there have been media reports of recent chikungunya deaths.
Source: National Vector Borne Disease Control Programme, Central Bureau of Health Intelligence
“We have no evidence to prove that chikungunya has killed people in India. Chikungunya- positive people who have died, died due to co-morbid conditions,” said Dr AC Dhariwal, former head of the NVBDCP to Hindustan times. However, more research is needed to conclusively rule out the possibility that the disease can kill patients, said Dr Saumya Swaminathan, director general of the Indian Council of Medical Research, in the same article.
Similarly there has been an increase in Japanese encephalitis, a viral brain fever spread by Culex mosquito that is seen more commonly in eastern India. In 2012, it affected 745 Indians, and the number grew to 1,676 in 2016. The number of deaths caused by the disease rose from 140 in 2012 to 283 in 2016.
Data, collected only from public health system, are misleading
NVBDCP is the primary source of information on vector-borne diseases but its figures may well be underestimated.
Figures collected from the medical cause of death certificates issued in Delhi showed that dengue fatalities were eight times higher than those stated by the NVBDCP, IndiaSpend reported in November 2016.
Even in Mumbai, there were 103 deaths due to malaria in 2014-15, according to medical cause of death data from municipal records accessed by Praja Foundation. But the NVBDCP data showed only 68 deaths due to malaria in the whole state of Maharashtra.
For its data, NVBDCP is dependent on monitoring and surveillance by primary health centres, malaria clinics, community health centres and secondary and tertiary-level health institutions. It misses figures from the private sector where a majority of the population seeks care.
Malaria has been made a notifiable disease in the national strategic plan for its elimination. This means that doctors in government, private and other formal settings have to notify the state of all cases of malaria. This may improve the surveillance and quality of data.
“We are currently reporting malaria figures only from the public health system” said Neeraj Dhingra, additional director, NVBDCP. “We are requesting states to make malaria notifiable so that we get figures from the private sector as well.”
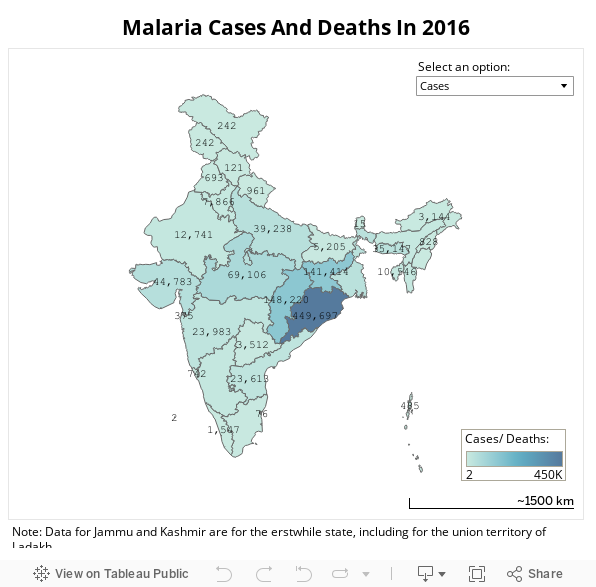
Tribals, 8% of total population, account for 70% malarial deaths
Inaccessible regions of India, such as tribal and mountainous belts, where only 20% of Indians live, report 80% of malaria cases, according to the NVBDCP.
Chhattisgarh, Jharkhand, Madhya Pradesh and Orissa together had 74% of all malaria cases in 2016.
“Even though the tribal population is 8% of India’s total population, it accounts for 70% of malarial deaths,” said Sushil Patil, clinical coordinator, Jan Swasthya Sahyog, a non-profit organisation that provides low-cost health care in the tribal areas of Bilaspur in Chhattisgarh.
He said the forested tribal areas in India see more of the plasmodium falciparum strain of malaria which is more likely to cause complications. But patients here have to deal with poor access to diagnostics and treatment. “A PHC reporting a malarial death is seen to be working poorly by higher ups, so there is no incentive to report deaths,” Patil added.
There is a shortage of staff and sanctioned posts for health workers and programme staff throughout the country. There are 40,000 multipurpose workers against 80,000 posts sanctioned for nearly 150,000 sub-centres in the country, noted national strategic plan. “There is a shortage of qualified entomologists (experts in insects) in the country leading to poor vector surveillance and lack of robust data on entomological aspects of malaria,” the report said.
Migration and drug resistance add to the challenge
Large-scale migration of populations from one state to another also makes malaria management difficult. Each state has a different quality of healthcare which makes it difficult to control the spread of the disease as people move.
India also shares its borders with Myanmar and Bangladesh, both malaria-endemic and this means high chances of malaria influx.
Another challenge is the resistance of mosquitoes to drugs and insecticides. The excessive use of DDT has already made An. Culicifacies mosquito resistant to it.
Plasmodium falciparum was first detected to be resistant to chloroquine, the cheapest anti-malarial drug, in 1973. Since 2002, many vulnerable regions with falciparum malaria are using the artemisinin combination therapy (ACT) to deal with the disease.
